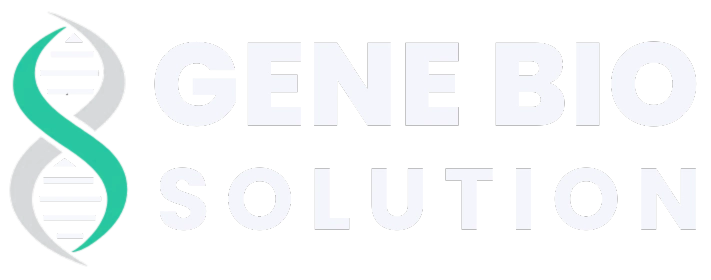
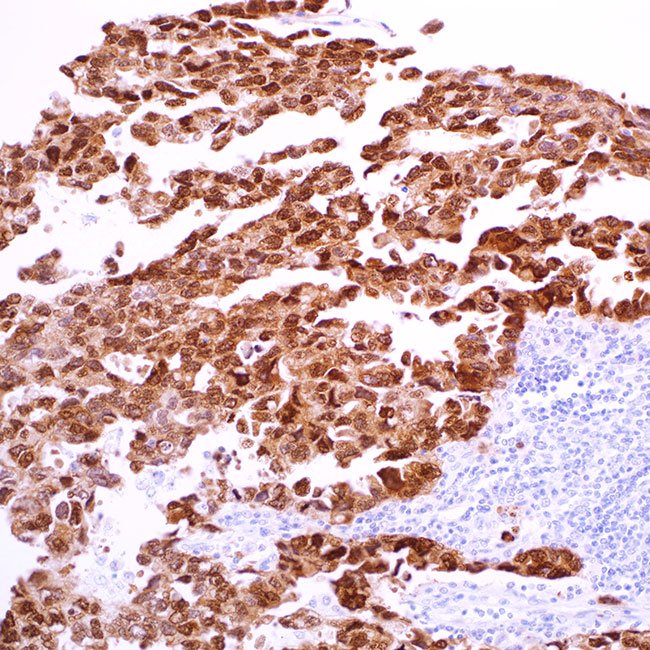
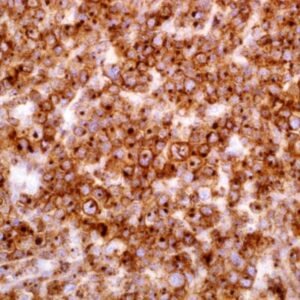
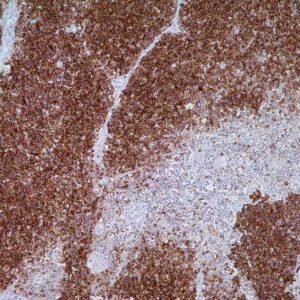
Distinguishing seminomas from non-seminomatous germ cell tumors can be difficult, particularly when dealing with small biopsy samples, necrotic tumors, and metastatic tumors that show artifacts. A particular group of germ cell tumors might need immunohistochemistry (IHC) for proper classification due to atypical morphological traits, like the widespread growth of clear cells and tumors exhibiting glandular or microcytic patterns. In a mixed germ cell tumor, one part frequently intertwines closely with others, like embryonal carcinoma and yolk sac tumor, potentially going unnoticed. IHC can pinpoint such regions, allowing more precise identification of each component within the mixed tumor, and the WHO recommends recording them in pathology reports. Recent IHC research has indicated that the combination of CD30 and CD117 staining is effective in differentiating between embryonal carcinoma and yolk sac tumor. Nevertheless, some tumors may not be easily distinguished using this pair of markers. Furthermore, the typical membranous pattern created by antibodies to CD30 and CD117 used for diagnostic interpretations may not appear clearly in small biopsy samples. In this regard, transcription factors, such as SOX-2, are simpler to interpret because of their distinct nuclear reactions. SOX-2 has been identified as a diagnostic marker for embryonal carcinoma. In fact, SOX-2 was found in all cases of intratubular embryonal carcinoma, pure embryonal carcinoma, and in the embryonal carcinoma portion of mixed germ cell tumors. However, SOX-2 expression has generally not been observed in seminomas, yolk sac tumors, or choriocarcinomas. Including transcription factors like SOX-2 and SOX-17 in an IHC panel aids in the classification of germ cell tumors: specifically, SOX-2+/OCT3/4+/CD30+/CD117-/SOX17- indicates embryonal carcinoma; SOX-2-/OCT3/4+/CD30-/CD117+/SOX17+ indicates seminoma; and SOX-2-/OCT3/4-/CD30-/CD117-/SOX17- indicates yolk sac tumor.